
Cytomegalovirus (CMV) Retinitis
Bottom Line Up Front: Cytomegalovirus (CMV) retinitis is a serious viral infection of the retina that primarily affects immunocompromised individuals. Without prompt treatment, this condition can lead to permanent vision loss or blindness. Early detection through regular ophthalmologic examinations and immediate antiviral therapy are essential for preserving sight in patients with CMV retinitis.
What is Cytomegalovirus (CMV) Retinitis?
Cytomegalovirus retinitis (CMV retinitis) is a sight-threatening viral infection that attacks the retina—the light-sensitive neural tissue lining the posterior wall of the eye. This condition predominantly affects patients with compromised immune systems and represents one of the most serious ocular complications in immunocompromised individuals.
Cytomegalovirus (CMV) belongs to the herpesvirus family and maintains lifelong latency in approximately 60-90% of adults worldwide, with prevalence varying by geographic region and socioeconomic factors. While immunocompetent individuals typically harbor the virus asymptomatically, viral reactivation can occur when immune surveillance becomes impaired, potentially causing devastating retinal damage.
Historical Context and Current Landscape
CMV retinitis gained clinical prominence during the HIV/AIDS epidemic of the 1980s and 1990s, when it emerged as the leading cause of blindness in patients with advanced immunodeficiency. Although modern antiretroviral therapy has reduced its incidence by over 80% in HIV-positive patients, the condition remains a significant clinical challenge among diverse immunocompromised populations, including:
- Solid organ and hematopoietic stem cell transplant recipients
- Patients receiving intensive cancer chemotherapy
- Individuals on chronic immunosuppressive therapy for autoimmune conditions
- Recipients of high-dose corticosteroid treatment
The epidemiologic landscape has evolved substantially, with non-HIV immunocompromised patients now representing an increasing proportion of CMV retinitis cases, particularly in developed nations where HIV care has advanced significantly.
Clinical Presentation of Cytomegalovirus (CMV) Retinitis
Early Clinical Manifestations
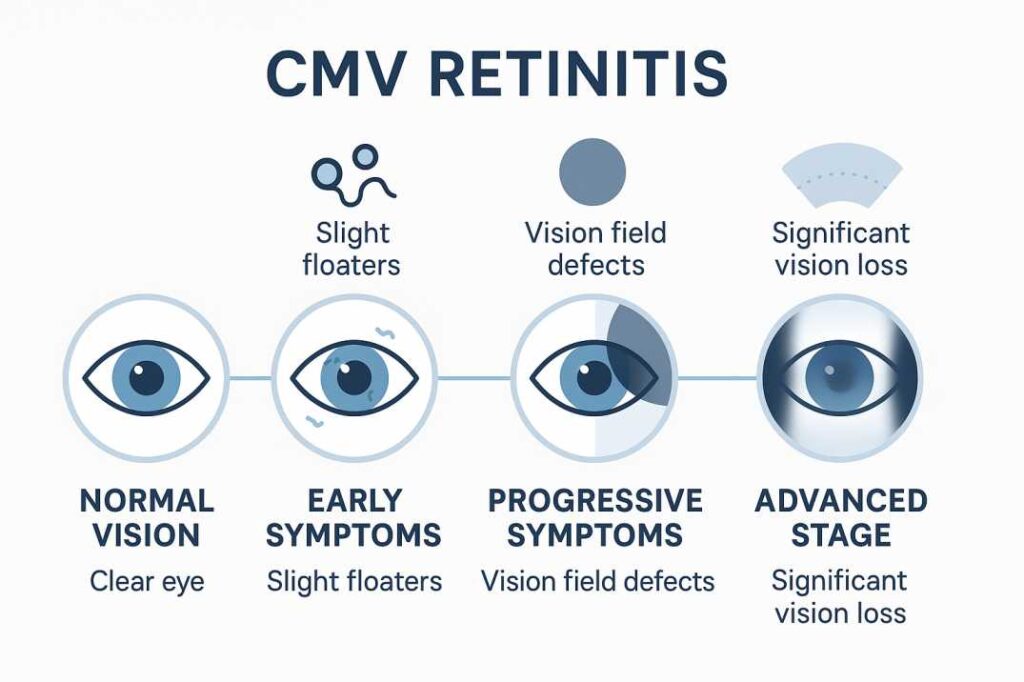
The initial presentation of CMV retinitis is often insidious, with patients frequently remaining asymptomatic during early stages of retinal involvement. When symptoms do manifest, they typically include:
Visual Disturbances:
- Progressive increase in vitreous floaters (muscae volitantes)
- Gradual deterioration of visual acuity over days to weeks
- Peripheral visual field defects (scotomata)
- Metamorphopsia (visual distortion)
- Photopsias (subjective light flashes)
Clinical Pearl: The absence of pain distinguishes CMV retinitis from many other inflammatory ocular conditions, though this painless progression often delays patient presentation and diagnosis.
Disease Progression and Pathognomonic Features
Without therapeutic intervention, CMV retinitis follows a predictable pattern of centripetal spread from peripheral retinal foci toward the posterior pole. The classic ophthalmoscopic findings include:
Fundoscopic Characteristics:
- Confluent areas of full-thickness retinal necrosis with a distinctive “cottage cheese and ketchup” or “pizza” appearance
- Granular satellite lesions at the advancing border of infection
- Perivascular retinal hemorrhages and exudates
- Retinal vasculitis with characteristic perivascular sheathing
- Minimal to absent vitreous inflammation (reflecting profound immunosuppression)
Anatomic Patterns: The clinical presentation varies based on the predominant pattern of retinal involvement:
- Hemorrhagic type: Extensive posterior involvement with prominent bleeding and edema
- Granular type: Peripheral distribution with less dramatic inflammatory changes
- Frosted branch angiitis pattern: Distinctive perivascular white infiltrates mimicking other inflammatory conditions
Who’s at Risk for Cytomegalovirus (CMV) Retinitis?
High-Risk Populations
HIV/AIDS Patients:
- The greatest risk occurs when CD4+ cell counts drop below 50 cells/μL
- Risk increases dramatically without effective antiretroviral therapy
- Historically, it affected 20-30% of AIDS patients before modern treatments
Transplant Recipients:
- Solid organ transplant patients on immunosuppressive medications
- Bone marrow/hematopoietic stem cell transplant recipients
- Recent studies show that 11.3% of patients with CMV viremia develop retinitis after transplantation
Cancer Patients:
- Those undergoing chemotherapy
- Patients with blood cancers like leukemia or lymphoma
- Individuals receiving radiation therapy
Other Immunocompromised Conditions:
- Autoimmune diseases requiring immunosuppressive therapy
- Chronic corticosteroid use
- Congenital immunodeficiency disorders
Current Incidence in the HAART Era
Modern data shows CMV retinitis now occurs at a rate of approximately 0.36-5.6 per 100 person-years in AIDS patients, representing a dramatic decrease from pre-HAART rates of 20 per 100 person-years. However, new cases continue to occur, particularly in:
- Local immunosuppression: Patients receiving intravitreal corticosteroid injections
- COVID-19 complications: Some cases report CMV reactivation following severe COVID-19 infections
- Age-related immune decline: Elderly patients may develop atypical presentations
Contemporary Diagnostic Approaches for CMV Retinitis
Clinical Assessment Protocol
Comprehensive Ophthalmologic Examination: The diagnosis of CMV retinitis remains predominantly clinical, based on characteristic fundoscopic findings in an appropriate immunologic context. Essential examination components include:
- Medical history review: Comprehensive assessment of immunosuppressive conditions, CD4+ counts, transplant status, and current medications
- Best-corrected visual acuity testing: Baseline measurement for monitoring treatment response
- Dilated indirect ophthalmoscopy: Visualization of the peripheral retina, where lesions commonly originate
- Digital fundus photography: Documentation of lesion characteristics and extent for serial monitoring
Laboratory Confirmation Strategies
Molecular Diagnostic Testing: When clinical diagnosis remains uncertain or treatment monitoring is required:
- Polymerase Chain Reaction (PCR): Aqueous or vitreous humor sampling for CMV DNA detection
- Quantitative viral load assessment: Correlation between intraocular viral burden and disease activity
- Resistance mutation analysis: UL97 and UL54 gene sequencing for patients with treatment failure
Systemic Evaluation:
- CD4+ T-lymphocyte count: Critical for risk stratification and screening interval determination
- Plasma CMV viral load: May correlate with ocular disease risk in certain populations
- CMV serology: Historical exposure assessment, particularly relevant in transplant recipients
Screening Recommendations
Evidence-Based Screening Intervals:
- CD4+ counts below 50 cells/μL: Ophthalmologic evaluation every 3 months (incidence rate of 3.89 per 100 person-years)
- CD4+ counts 50-100 cells/μL: Semi-annual comprehensive eye examinations
- Recent transplant recipients: Monthly monitoring for 6-12 months post-transplantation
- High-dose corticosteroid therapy: Baseline examination with periodic follow-up based on duration and dosage
At Cannon EyeCare, we recommend that all immunocompromised patients establish baseline retinal imaging and maintain regular monitoring schedules tailored to their specific risk profiles and immune status.
Treatment Options for Cytomegalovirus (CMV) Retinitis
Immediate Treatment Goals
- Stop viral replication and retinal damage
- Preserve remaining vision
- Prevent spread to the unaffected eye
- Address underlying immune system issues
Antiviral Medications
First-Line Treatments:
Valganciclovir (Oral):
- Most commonly prescribed initial treatment
- Convenient oral administration
- Effective for both induction and maintenance therapy
- Requires monitoring for bone marrow suppression
Ganciclovir:
- Available as an intravenous or intravitreal injection
- Faster onset for severe cases
- Direct injection provides higher retinal concentrations
- May cause neutropenia (low white blood cell count)
Second-Line Options:
Foscarnet:
- Used when resistance to ganciclovir develops
- Available intravenously or as an intravitreal injection
- Alternative for patients with drug-induced neutropenia
- Requires careful kidney function monitoring
Cidofovir:
- Reserved for resistant cases
- Administered intravenously
- Significant nephrotoxicity risk
Emerging Therapies
Recent studies from 2024-2025 have shown promising results with newer antiviral agents:
Letermovir and Maribavir:
- Novel mechanisms of action
- Particularly effective for resistant CMV strains
- Better tolerance profiles in some patients
- Currently being studied for retinitis applications
Surgical Interventions
When Surgery May Be Necessary:
Retinal Detachment Repair:
- Occurs in approximately one-third of CMV retinitis patients
- Vitrectomy with silicone oil or gas tamponade
- Success rates of 56-94% for reattachment
- Better outcomes when performed early
Ganciclovir Implants:
- Sustained-release intraocular devices
- Last 6-8 months per implant
- Provide high local drug concentrations
- Useful for patients intolerant of systemic therapy
Managing Underlying Conditions
Critical Component of Treatment:
- HIV patients: Highly Active Antiretroviral Therapy (HAART)
- Transplant recipients: Optimizing immunosuppression levels
- Cancer patients: Coordinating with the oncology team
- General immune support: Addressing nutritional deficiencies
Complications and Long-Term Outcomes
Potential Complications
Retinal Detachment:
- Occurs in approximately 11% of CMV retinitis patients (recent 2024 meta-analysis)
- Previously cited rates of 25-33% may have been overestimated
- Requires immediate surgical intervention
- Strong predictor of poor visual outcomes
Immune Recovery Uveitis (IRU):
- Paradoxical inflammation following immune system recovery
- Common in HIV patients starting HAART
- May cause additional vision loss
- Requires anti-inflammatory treatment
Drug Resistance:
- Develops with prolonged antiviral therapy
- Mutations in viral genes UL97 and UL54
- May require alternative medications
- Regular monitoring through PCR testing
Visual Prognosis
Factors Affecting Outcomes:
- Location of lesions: Central involvement has a worse prognosis
- Extent of retinal damage: Larger areas of necrosis predict poorer vision
- Timing of treatment: Earlier intervention preserves more vision
- Immune system recovery: Better outcomes with improved immunity
Recovery Expectations:
- Vision lost to CMV retinitis cannot be restored
- Treatment aims to prevent further damage
- Visual acuity improvement occurs in approximately 18% of patients with treatment
- Inflammation resolution achieved in 90% of cases with antiviral therapy
- Disease recurrence occurs in about 19% of treated patients
- Regular monitoring is required lifelong
Prevention and Screening
Preventive Strategies
For High-Risk Individuals:
- Regular eye examinations based on immune status
- Prompt treatment of underlying conditions
- Prophylactic antiviral therapy in select cases
- Avoiding additional immunosuppression when possible
Screening Guidelines:
- CD4+ count <50: Every 3 months
- CD4+ count 50-100: Every 6 months
- Recent transplant: Monthly for first 6 months
- High-dose steroids: Baseline and periodic follow-up
Patient Education Points
When to Seek Immediate Care:
- Sudden increase in floaters
- New blind spots or vision loss
- Flashing lights
- Curtain or shadow in peripheral vision
- Any vision changes in immunocompromised patients
The Role of Telemedicine and Modern Screening
Innovative Approaches
Recent developments include:
- Remote fundus photography for screening in underserved areas
- AI-assisted diagnosis for early lesion detection
- Smartphone-based monitoring for symptom tracking
- Telemedicine consultations for rural patients
Cost-Effective Screening
Studies demonstrate that regular screening programs, even in resource-limited settings, significantly reduce blindness rates and improve quality of life for at-risk populations.
Research Updates and Future Directions
Recent Scientific Advances (2024-2025)
Immunotherapy Developments:
- CMV-specific adoptive T-cell therapy
- CMV immunoglobulin (CMVIG) treatment
- Reduced mortality and improved tolerance compared to traditional antivirals
Drug Resistance Management:
- Better understanding of resistance mutations
- Combination therapy approaches
- Newer antiviral agents with different mechanisms
Personalized Treatment:
- Genetic testing for drug metabolism
- Tailored therapy based on viral genetics
- Immune status-guided treatment duration
Emerging Challenges
Non-HIV Populations:
- Increasing recognition in transplant recipients
- Different clinical presentations compared to HIV patients
- Need for specialized management protocols
Global Health Considerations:
- Persistent high incidence in developing countries
- Limited access to advanced treatments
- Need for simplified screening and treatment protocols
Key Takeaways for Patients with Cytomegalovirus (CMV) Retinitis
Essential Points to Remember:
- Early detection saves vision – Regular eye exams are crucial for high-risk individuals to prevent cytomegalovirus retinitis progression
- Treatment prevents progression – Prompt antiviral therapy can preserve remaining sight in CMV retinitis cases
- Immune system health matters – Managing underlying conditions is equally important for cytomegalovirus retinitis outcomes.
- Vision loss is permanent – Prevention and early intervention are the best strategies for CMV retinitis.s
- Long-term monitoring required – Cytomegalovirus retinitis can recur even after successful treatment
Questions for Your Eye Care Provider:
- What is my personal risk level for cytomegalovirus (CMV) retinitis based on my current immune status?
- How often should I have ophthalmologic examinations to screen for CMV retinitis?
- What specific symptoms of cytomegalovirus retinitis should prompt immediate evaluation?
- Are there any preventive measures I should take against CMV retinitis, given my medical conditions?
- How will my other medical treatments affect my cytomegalovirus retinitis risk profile?
For patients in the Seattle area, Cannon EyeCare maintains expertise in managing complex retinal conditions in immunocompromised patients, with specialized protocols for CMV retinitis screening and treatment coordination.
When to Seek Eye Care for CMV Retinitis Symptoms
Immediate Consultation Needed
Contact an ophthalmologist immediately if you experience:
- Sudden onset or worsening of visual symptoms
- New or increasing floaters, especially with flashing lights
- Progressive visual field defects or blind spots
- Any ocular symptoms in the context of known immunocompromise
The specialists at Cannon EyeCare in Seattle provide comprehensive evaluation and management for patients with suspected or confirmed CMV retinitis, utilizing advanced diagnostic imaging and maintaining close collaboration with infectious disease specialists and transplant teams.
Regular Monitoring Protocol
High-risk patients should maintain:
- Scheduled ophthalmologic examinations based on immune status and risk stratification
- Coordinated communication between all healthcare providers (ophthalmology, infectious disease, primary care)
- Updated vaccination status where medically appropriate
- Comprehensive documentation of all medications and immunosuppressive treatments
Cannon EyeCare works closely with Seattle-area infectious disease specialists, transplant centers, and oncology practices to ensure seamless care coordination for patients requiring long-term CMV retinitis monitoring and management.
Living with CMV Retinitis: A Comprehensive Approach
Quality of Life Optimization
Vision Rehabilitation Services:
- Low vision assessment and adaptive technology training
- Occupational therapy for daily living skills
- Support group participation and peer counseling
- Educational resources for patients and families
Medication Management Excellence:
- Understanding potential side effects and drug interactions
- Adherence strategies for complex treatment regimens
- Regular laboratory monitoring coordination
- Communication protocols with the healthcare team
At Cannon EyeCare, our patient care coordinators work with Seattle-area low vision specialists and rehabilitation services to ensure patients have access to comprehensive support resources throughout their treatment journey.
Long-term Care Planning:
- Regular ophthalmologic follow-up
- Coordination with other specialists
- Emergency action plans
- Family education and support
Essential Resources and Expert Citations
1. National Institutes of Health (NIH) – Clinical Guidelines for CMV Disease
Why This Resource: The NIH provides the most current, evidence-based clinical guidelines for healthcare providers treating cytomegalovirus retinitis. Updated regularly with the latest research findings, this resource includes diagnostic criteria, treatment protocols, and monitoring recommendations. Essential reading for understanding current standard-of-care practices and treatment decisions.
Key Information Available:
- Current diagnostic standards and PCR testing protocols
- Comprehensive treatment algorithms for both HIV and non-HIV patients
- Drug resistance management strategies
- Monitoring schedules based on immune status
2. American Academy of Ophthalmology – Patient Education Resource
URL: https://www.aao.org/eye-health/diseases/what-is-cytomegalovirus-retinitis
Why This Resource: The AAO provides trusted, patient-friendly information that balances medical accuracy with accessibility. This resource is regularly reviewed by ophthalmology experts and updated to reflect current practice standards. Particularly valuable for patients seeking clear explanations of symptoms, treatment options, and what to expect during care.
Key Information Available:
- Clear symptom descriptions and progression patterns
- Risk factor identification for different patient populations
- Treatment overview, including surgical options
- When to seek immediate medical attention
3. 2024 Systematic Review – Survey of Ophthalmology
Full Citation: Putera, I., Nora, R.L.D., Dewi, A.C., et al. (2024). Antiviral therapy for cytomegalovirus retinitis: A systematic review and meta-analysis. Survey of Ophthalmology, 70(2), 215-231.
DOI: https://doi.org/10.1016/j.survophthal.2024.11.004
Why This Research: This comprehensive 2024 meta-analysis represents the most current evidence-based treatment outcomes data available. Analyzing 59 studies with 4,501 patients, it provides the most reliable statistics on treatment success rates, complication frequencies, and comparative effectiveness of different therapeutic approaches.
Key Findings Cited:
- Visual acuity improvement rates: 18% of patients
- Inflammation resolution: 90% with antiviral therapy
- Updated retinal detachment rates: 11% (lower than previously reported)
- Treatment recurrence rates: 19% across all therapies
These resources represent authoritative, peer-reviewed sources that form the medical foundation of this article. All treatment decisions should be made in consultation with qualified healthcare providers.
Conclusion: Integrating Modern CMV Retinitis Management
Cytomegalovirus retinitis remains a formidable clinical challenge requiring multidisciplinary expertise and vigilant monitoring. While advances in antiretroviral therapy have dramatically reduced the incidence of HIV-positive patients, the condition continues to threaten vision in diverse immunocompromised populations. The evolving landscape of transplant medicine, cancer therapy, and autoimmune disease management necessitates ongoing awareness among healthcare providers.
Early recognition through systematic screening programs, coupled with prompt initiation of appropriate antiviral therapy, offers the best opportunity for visual preservation. The integration of novel therapeutic agents, enhanced diagnostic techniques, and personalized treatment approaches promises continued improvement in patient outcomes.
For comprehensive ophthalmologic evaluation and specialized management of CMV retinitis, consultation with retinal specialists experienced in immunocompromised patient care is essential. Cannon EyeCare in Seattle provides expert evaluation and ongoing management for patients with CMV retinitis, utilizing state-of-the-art diagnostic technology and maintaining collaborative relationships with regional transplant centers, infectious disease specialists, and oncology practices.
The preservation of vision in CMV retinitis exemplifies the critical importance of collaborative care between ophthalmologists, infectious disease specialists, transplant physicians, and primary care providers. Through continued research, education, and clinical vigilance, we can optimize outcomes for patients facing this sight-threatening condition.
This information is for educational purposes and should not replace professional medical advice. Always consult with your healthcare provider for personalized recommendations.
FAQs
-
-
CMV retinitis is a serious viral eye infection that inflames the retina and can cause blindness, especially in people with weakened immune systems.
-


